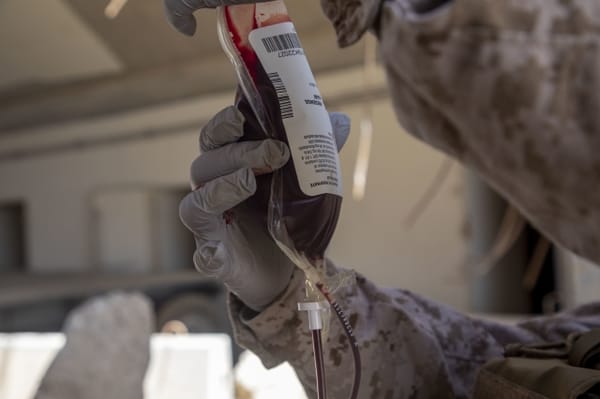
Bleed Ready Bleed‑Ready: lessons from Sydney’s terror attack Bleed Ready 14 Dec 2025 — 6 min read Australia, Bondi Beach Terror Attack - December, 2025